What is a Ligament?
A ligament is structure made of tough fibrous tissue supporting the joint. Ligaments are present both inside and outside a joint. The function of a ligament is to prevent excessive and abnormal movement of the bones of a joint relative to each other. A ligament thus gives stability to a joint. It follows therefore that injury to a ligament will cause some instability of the affected joint.
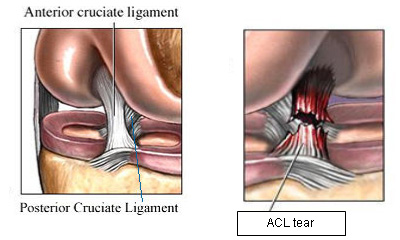
Which are the ligaments of the knee joint?
The knee joint has four main ligaments – two inside and two outside the joint. The ligaments outside the joint are called collateral ligaments. There are two collateral ligaments – (i) Medial collateral ligament (MCL) present on the inner aspect of the knee and (ii) Lateral collateral ligament (LCL) present on the outer aspect of the knee. The MCL prevents excessive outward bending and the LCL prevents excessive inward bending of the tibia on the femur.
The ligaments inside the joint are called Cruciate ligaments. There are two cruciate ligaments – (i) Anterior cruciate ligament (ACL) which is present in the front of the knee and (ii) Posterior cruciate ligament (PCL) which is present at the back of the knee. The ACL prevents excessive forward translation of the tibia on the femur and the PCL prevents excessive backward translation of tibia on femur. The ACL is more commonly injured than the PCL.
How is the ACL injured?
The ACL may be injured due to:
1) Pivoting injury – when a sudden twisting force is applied to a knee with the foot planted firmly on the ground
2) Deceleration injury – due to landing directly on the feet as in a fall
3) Direct injury – due to a direct blow to the knee as in a football or rugby tackle or a road traffic accident (RTA).
What are the symptoms of an ACL tear?
At the time of injury, patients may hear an audible “pop” in the knee followed by pain and swelling in the knee and inability to move the knee. When the initial pain and swelling settle down patients will complain of:
Buckling or “Giving way” of the knee
• Difficulty in bending or straightening the knee
• Catching or locking of the knee
• Repeated swelling (effusion) in the knee
• Pain (this usually indicates associated tear of the meniscus)
How is an ACL tear diagnosed?
The diagnosis is made on the basis of patient’s history of symptoms of giving way and physical examination. There are certain clinical tests like the Anterior Drawer’s test, Lachman’s test and Pivot shift test which point towards an ACL tear.

Lachman’s test for ACL Anterior drawer test for ACL tear
X-rays and MRI scan are two tests which are commonly employed in patients with ACL tears. X-rays are usually normal in a young patient with ACL tears. In middle-aged and older patients X-rays may reveal changes of arthritis. These changes will dictate whether a patient is treated surgically or not. MRI scanning is a sensitive test for detecting ACL tears. It will also reveal any associated injuries like meniscal tears and articular cartilage damage to the knee.
Do ACL tears heal by themselves?
An ACL tear can rupture at three different sites – 1) at it’s attachment to the thigh bone (femur), 2) through its substance (mid-substance tears) or 3) at it’s attachment to leg bone (tibia). Mid-substance ACL tears and those occurring at the femoral attachment generally do not heal by themselves. ACL tears occurring at the tibial attachment site frequently pull-off a piece of bone with it (ACL avulsion injuries). These tears have the potential to heal on their own provided the bony fragment is not displaced. In cases where the bony fragment is displaced, the ACL can be repaired by fixing the bony fragment back in its place along with the ACL.
Does every patient with an ACL tear need surgery?
Every patient with an ACL tear does not need surgical intervention. A proportion of patients do well with rehabilitation (physiotherapy). A proportion of patients will have some symptoms of instability (giving way) despite undergoing a good rehabilitation program but are able to manage with some life-style modifications. Those who continue to have disabling symptoms of instability will need surgery. This is particularly so with patients who are young, active or those involved with competitive sports or strenuous activity.
Treatment of ACL tears
In general the treatment options for ligament injuries of the knee can be summarized as follows:
1. Rest, Ice application, Compression, Elevation (RICE)
2. Braces
3. Physiotherapy
4. Surgery
NON-SURGICAL TREATMENT OF ACL TEARS
Almost all patients can be managed without surgery to begin with. This consists of rest, ice application, compression, elevation (RICE) until the pain and swelling settles down. This is followed by a comprehensive rehabilitation program (Physiotherapy) geared towards achieving range-of-motion (movement) in the knee, strength in the quadriceps and hamstring muscles, and knee joint stability. A hinged knee brace may be helpful in some patients.
SURGICAL TREATMENT OF ACL TEARS
Factors which need to be taken into consideration before considering a patient for surgery are:
1. Age of the patient
2. Patient’s activity level
3. Patient’s expectations
4. Patient’s ability and willingness to participate in the post-op rehabilitation program
5. Associated injuries like meniscal tears and collateral ligament injuries
6. Presence of osteo-arthritic changes in the knee.
Thus, a young active patient desirous of leading an active life-style or pursuing a sporting activity, those with associated with meniscal tear, and those who have persistent instability after non-operative treatment are all candidates for surgery.
Surgery for a torn ACL invariably involves an Arthroscopic reconstruction of the torn ligament (replacing the torn ligament with a biologic or artificial graft). Arthroscopic Repair of the torn ACL (stitching or suturing the torn ends together) does not achieve satisfactory healing and is considered only where the ligament tears off from the tibial side with a piece of bone.
The grafts used for ACL reconstruction are may be categorized as – Autografts (harvested from the patient himself), Allografts (harvested from cadavers), or Artificial grafts (synthetic grafts). Generally autografts (hamstring tendons or bone-patella-bone) are used in most cases. Allografts or artificial grafts are reserved for revision surgeries or in patients with multiple ligament injuries (combined ACL, PCL and collateral ligament injuries).
Choice of autograft to be used
The choice of the graft to be used depends upon the preference of the surgeon, the activity level of the patient, and on whether or not the patient has any patello-femoral pain (pain from the knee cap). The two most commonly used autografts are:
1. Hamstring tendon graft – either semi-tendinosus alone or semi-tendinosus and gracilis tendons taken together. These tendons are harvested with a small incision over shin bone close to the knee.
2. Bone-patella-bone (BTB) graft – involves taking part of the patella bone (knee cap), the patellar liagament and the tibial tuberosity (front of the leg bone). The graft is harvested with an incision over the front of the knee.
How is ACL surgery performed?
ACL surgery is performed as an arthroscopic surgery (key-hole surgery) using 2 or 3 portals (small cuts). Where a reconstruction is to be performed using an autograft, an additional small incision is required to harvest the graft. A diagnostic arthroscopy is first performed to evaluate the nature of ACL tear (partial or complete tear) and any associated injuries to the meniscus and the articular cartilage. The remnant of the torn ACL is removed using a device called the shaver. Two tunnels are made in the bones (tibia and femur) using specialized instruments called endoscopic jigs and reamers. The graft is prepared using a strong stitch like Ethibond to enable its passage through these bone tunnels. The graft is then fixed to bone using various different methods (interference screws, endobuttons, suture wheels, transfix device).

1. ACL reconstruction using Bone-patella-bone graft
2. ACL reconstruction using Hamstring tendon graft
3. Specialized endoscopic jig for Arthroscopic ACL reconstruction
Post-op Rehabilitation after ACL reconstruction
These surgeries can be performed as “day care surgery” where the patient is discharged the same day. It is however common to keep the patient in the hospital for a couple of days after surgery for pain relief and immediate post-operative rehabilitation. The rehabilitation protocols vary from surgeon to surgeon, and also depend on the type of graft used and the associated injuries. In general, most patients are advised to wear a brace of some description for a period of 2-4 weeks. Patients are allowed to walk almost immediately after surgery using a brace and crutches. Patients are given an exercise program for muscle strengthening and achieving movement in the knee.
How long does it take to recover from an ACL reconstruction surgery?
The recovery time after ACL surgery varies from patient to patient, and depends on the level of activity the patient wants to pursue after surgery. In general it takes about 2-3 months for most patients to recover completely from the surgery. Those desirous of engaging in competitive sports or other high demand activity may need a longer and a more specific rehabilitation program.
What is outcome of ACL reconstruction surgery?
ACL surgery is considered as a ‘high yield surgery’ considering the high rates of success and low rates of complications. The overall success rates after this surgery are very high.
90% of patients are able to return to their work or activity as before the injury. Some patients report a feeling that knee does not feel absolutely normal though they may be able to perform their activities without any hindrance.
Are there any risks and complications associated with ACL reconstruction?
The overall complication rates are low. The possible risks and complications are:
1. Infection
2. Deep Vein Thrombosis (DVT)
3. Arthrofibrosis (Stiffness)
4. Graft rupture
New Developments in ACL surgery
What is Double Bundle (Anatomic) ACL reconstruction?
It is a well known fact that the normal ACL is made up of two functional bundles – the antero-medial (AM) bundle and the postero-lateral (PL) bundle. The AM bundle of the ACL primarily controls anterior (forward) movement of the tibia on the femur, and the PL bundle controls rotational stability of the knee, such as in pivoting, twisting, running, and jumping.

Double bundle reconstruction aims to restore both the anatomy and the function of the ACL. This technique involves making two bony tunnels each in the femur and tibia, and making two bundles of graft and passing them separately through these tunnels. The current technique involves harvesting both hamstring tendons (semi-tendinosus and gracilis).

Single bundle ACL reconstruction Double bundle ACL reconstruction
tional bundles – the antero-medial (AM) bundle and the postero-lateral (PL) bundle. The AM bundle of the ACL primarily controls anterior (forward) movement of the tibia on the femur, and the PL bundle controls rotational stability of the knee, such as in pivoting, twisting, running, and jumping.
Does double bundle ACL reconstruction give better results than conventional (single bundle) ACL reconstruction?
Conventional single bundle reconstruction is known to give good results with nearly 80-90% of patients being able to return to their pre-operative activity levels. On the other hand it is also known that around 10-30% of the patients who have undergone conventional ACL surgery, have some persistent instability after surgery. It is considered by some authors that a double bundle reconstruction would address this shortcoming. Though initial results are encouraging, it remains to be seen if long-term results of double bundle surgery would be better than conventional single bundle surgery.